Cervical Disc Replacement And \ Or Fusion
Introduction
An anterior cervical decompression is an operation performed for arm pain due to a pinched nerve in the neck, or for spinal cord compression in the neck. In order for it to be successful there has to be good evidence of nerve and/or spinal cord compression in the neck (preferably with an MRI scan as seen below), pain, weakness, or numbness in the arm corresponding to the MRI findings, no evidence of superimposed carpal tunnel syndrome or ulnar nerve compression, and clinical evidence of cervical myelopathy in some cases.
operation codes
For the purposes of your medical insurance you may need to quote the following codes to your insurer for pre-authorisation of treatment
V2950 Anterior Cervical Decompression and Fusion – 1-2 Levels
V2282 Anterior Cervical Discectomy and arthroplasty (joint replacement)
V2902 Revision Anterior Cervical Decompression and Fusion

This picture below , also seen also in the ‘arm pain’ section although in this case demonstrates a compressed cervical nerve root and the spinal cord due to a prolapsed cervical disc (upper arrow) and ‘wear and tear’ changes also called cervical spondylosis (lower arrow)
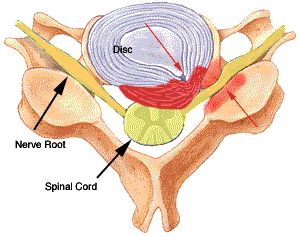
When performing an anterior cervical decompression, the entire cervical disc and the excess bone formed by wear and tear in the spine is removed in the region of the upper red arrow.
This is performed with the aid of a microscope, specialised instruments, and a high speed drill. This leads to the spinal cord and nerve root being decompressed.
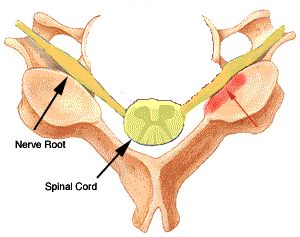
In the image above the disc prolapse and associated excess bone have been removed, leaving the spinal cord and nerve roots decompressed. There is still some posterior degenerative change,however, because the nerve root has been well decompressed from the front this bone does not need to be removed
The Operation
The operation is performed under a general anaesthetic
You will be lying on your back during the surgery. Your head will be supported by a jelly support. A small skin incision is made in a skin crease in the collar region on the right side of your neck, this incision is usually about 2-3cm long. The skin in this region heals very well and these incisions are barely visible a few weeks after surgery. The muscles in the neck run vertically and thus they can be split rather than cut. The surgery involves gently pushing the carotid artery and jugular vein to the side in order to get to the spine, also the voicebox (larynx) and pharynx/ oesophagus need to be gently pushed away from in front of the spine. Once the spine is in view a needle is placed in the suspected disc and an X-ray is taken to make sure we have selected the correct disc to remove.

The disc is then removed with special instruments and a drill using a microscope to magnify the view. Eventually the spinal cord coverings are seen, as are the nerve roots as they leave the spine at this level.
Bone and disc is removed until we are sure that these structures are decompressed
Fusion or Disc replacement?
Once the decompression has been performed debate exists about whether a fusion or a disc replacement should be performed, and what material/ implant is used to perform the fusion/ disc replacement.My own preference is wherever possible to use an artificial disc or disc replacement rather than perform a fusion. There is some evidence that replacing the disc rather than performing a fusion can improve neck pain after surgery, speed the recovery from surgery, and possible reduced the wear and tear at the discs above and below the level of surgery. The suitability for a disc replacement does depend on a number of factors though, and this option may not be the best choice for all patients.
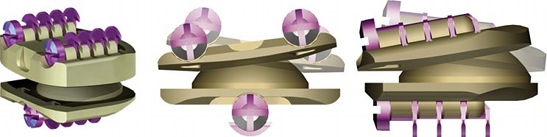
Above is a new implant called the NuNec which is virtually invisible on MRI as it is made of a polymer
Below is a video explaining the technique in performing a disc replacement using a nunec disc replacement.
I now use these disc replacements exclusively as the results are very good, and they do not interfere with the quality of MRI scans in the future.
In addition this this I run a UK based operative and lecture based course for spinal surgeons wishing to gain experience of this disc replacement, and teach on a similar course in Amsterdam.
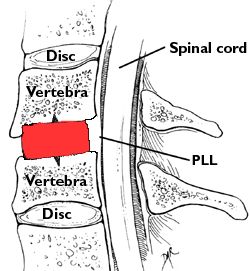
A disc replacement is not always appropriate and thus a fusion may be performed in some patients. Traditionally when a fusion was performed patients own bone in the form of a graft from the iliac crest (hip) was taken and placed at the site of the decompression. This however is a painful procedure, and the hip pain can persist long after the neck operation has settled down. When performing a fusion own preference is to use a ‘cage’, this is made of a polymer which integrates with your own bone, and to aid fusion is packed with bone fragments produced during the decompression. The image below shows a Solis cage.

The cage (red) is impacted at the site of surgery, and remains tightly in place due to a good fit (determined by templates), and small titanium pins anchoring the cage in bone
Recovery From Surgery
There is no need to wear a collar after surgery. Because the operation involves stripping a small area of muscle from the spine, the commonest problem is mild neck pain and stiffness after surgery. This pain tends to be mild and is easily controlled with painkilling medication such as ibuprofen. A drain is usually placed at the site of surgery, and removed first thing in the morning after the operation. Because the nerve root is manipulated during the operation, there may be some symptoms of tingling and numbness in the affected arm, and rarely the arm pain may return a couple of days after the operation as the nerve root can swell up. This is invariably a transient event and these symptoms will settle down as the nerve root swelling reduces, this incidence of this phenomenon has reduced markedly with the use of topical steroids. Very occasionally patients suffer with a hoarse voice and difficulty in swallowing, this usually settles within 48 hours
The incision is closed with dissolving stitches and thus you will not need to have any stitches removed
In almost all cases patients are able to go home within 24 hours of surgery. Recovery using modern techniques is so rapid we are currently exploring the option of patients going home the same day as surgery.
You can return to work when you fell comfortable, clearly this will depend upon how physically demanding your job is. In most cases 7-10 days off work is sufficient, if your job is physical then you may need up to 6 weeks off work. The DVLA state that you can drive when sufficiently recovered from surgery, in practical terms this means being able to look side to side and operate the car controls safely
Results Of Surgery
The results of surgery are good with a 90+% rate of improving the arm pain due to a compressed nerve root
The operation is not aimed at improving neck pain, but can improve neck pain in cases of instability/abnormal motion due to a particular disc space. For cases of cervical myelopathy (spinal cord compression), the results of surgery depend upon the severity of the spinal cord compression, your age, and how long the spinal cord has been compressed. Many patients with cervical myelopathy improve significantly, in some cases the operation stops further progression of the disease
The risks of surgery include, but are not limited to:
- The risks of a general anaesthetic ( this depends on your age and general health)
- Postoperative haematoma ( a drain is left in the wound for 24 hours after surgery)
- Failure to improve your arm pain (less than 10% of cases)
- Failure to improve cervical myelopathy
- Continued deterioration of spinal cord despite successful surgical decompression ( poorly understood and not common)
- Leakage of spinal fluid from the spine (less than 1%)
- Infection (1-2%)
- Damage to the nerve root or spinal cord (very rare, in the order of 1 in 1000-2000)
- Late instability of the spine ( rare, more common in multiple foraminotomies, or previous surgery to the spine)
- Non-union of the fusion site when performing a fusion
- Fusion of a cervical disc replacement (cessation of movement)