Cervical Foraminotomy
Introduction
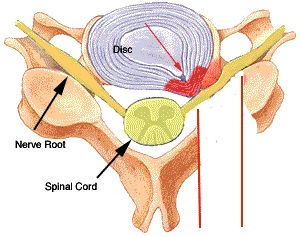
A posterior cervical foraminotomy is an operation performed for arm pain due to a pinched nerve in the neck. In order for it to be successful there has to be good evidence of nerve compression in the neck (preferably with an MRI scan), pain, weakness, or numbness in the arm corresponding to the MRI findings, and no evidence of superimposed carpal tunnel syndrome or ulnar nerve compression This picture seen below also in the ‘arm pain’ section demonstrates a compressed cervical nerve root either by a prolapsed cervical disc (upper arrow) or ‘wear and tear’ changes also called cervical spondylosis (lower arrow)
operation codes
For the purposes of your medical insurance you may need to quote the following codes to your insurer for pre-authorisation of treatment
V2200 Posterior Cervical Decompression (laminectomy) – 1-2 Levels
V2200 Posterior Cervical Foraminotomy – 1-2 Levels
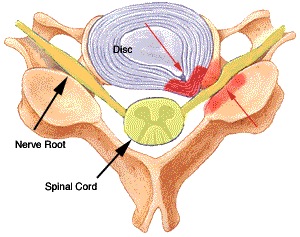
When performing a cervical foraminotomy, the excess bone formed by wear and tear in the spine is removed in the region of the lower red arrow. This is performed with the aid of a microscope, specialised instruments, and a high speed drill. This leads to the nerve root being decompressed. Because the canal where the nerve runs ( neural foramen) has had its roof removed there is no need to remove the compression from the front of the nerve root
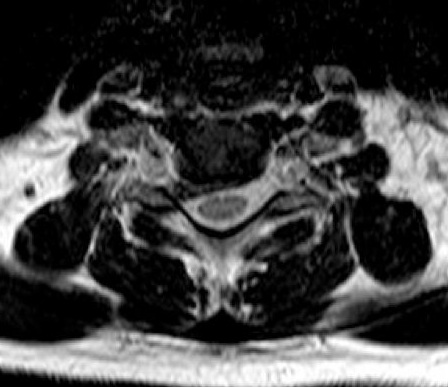
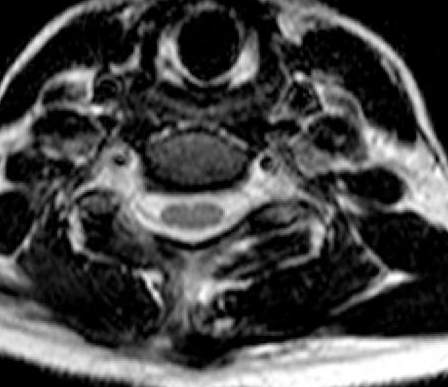
The images below are MRI scans showing the ‘before and after’ following a right C6 nerve root decompression via a posterior cervical foraminotomy. Hopefully it is clear that spinal fluid (white) is now visible around the nerve root confirming it has been decompressed on the second image.
The Operation
The operation is performed under a general anaesthetic
You will be lying on your front during the surgery. We need to keep your head very still during surgery and thus your head will be fixed rigidly in a head clamp, this may leave some tiny scratches on the side of your head hidden by your hair
An XRay will be taken to localise very closely the site of surgery, this allows a very small skin incision to be made just over the nerve root to be decompressed. For a single nerve root the incision is usually 16-18mm long.
Previously, in order to get to the spine the muscle overlying the facet joint to be partly removed needs to be separated from the bone of the spine. This has now changed and I have adopted a new technique using a keyhole surgery method. This uses a series of dilators to dilate a tract in the muscle, and the operation is performed via a small tube. This means a much smaller incision than previously, and less muscle trauma, and hence less neck pain after surgery.

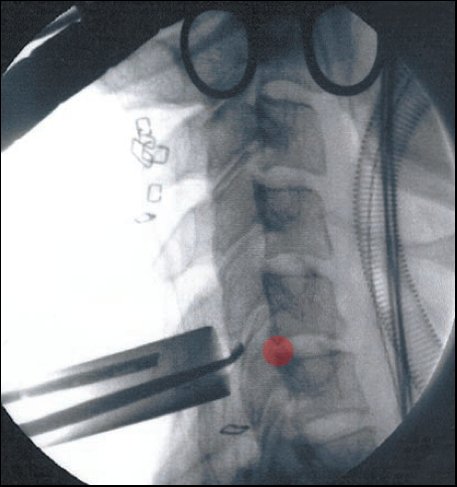
The image below has been taken during an operation. The tube can be seen passing from the skin to the spine, the red area represents approximately the area where a nerve root would be trapped.
Once the facet joint has been exposed by separating the muscle from it, the medial 1/3 to 1/2 of the facet joint is drilled away under a microscope. The final part of the facet joint in contact with the nerve root is removed with some fine bone rongeurs. At the end of the procedure the canal where the nerve exits the spine is probed to make sure it is free, and the nerve root is bathed in some steroid medication
Recovery From Surgery
This operation has the benefit of not affecting the mobility or stability of the cervical spine. This is because the disc is not removed and thus a fusion is not required, thus there is no need to wear a collar after surgery and there are no X-rays needed. Because the operation involves stripping a small area of muscle from the spine, the commonest problem is mild neck pain and stiffness after surgery. This pain tends to be mild and is easily controlled with painkilling medication such as ibuprofen. Because the nerve root is manipulated during the operation, there may be some symptoms of tingling and numbness in the affected arm, and rarely the arm pain may return a 7-10 days after the operation as the nerve root can swell up in response to the operation. This is invariably a transient event and these symptoms will settle down as the nerve root swelling reduces, this incidence of this phenomenon has reduced markedly with the use of topical steroids
The incision is closed with dissolving stitches and thus you will not need to have any stitches removed
In most cases patients are able to go home the day after surgery, or occasionally the same day
You can return to work when you fell comfortable, clearly this will depend upon how physically demanding your job is. In most cases 10-14 days off work is sufficient, if your job is physical then you may need up to 6 weeks off work. The DVLA state that you can drive when sufficiently recovered from surgery, in practical terms this means being able to look side to side and operate the car controls safely
Results Of Surgery
The results of surgery are good with a 90+% rate of improving the arm pain due to a compressed nerve root
The operation is not aimed at improving neck pain, this is because the neck pain usually originated from the degenerative changes in the spine and the changes due to wear and tear cannot be reversed with surgery. Some neck pain due to muscle spasm may well improve however
The risks of surgery include, but are not limited to:
- The risks of a general anaesthetic ( this depends on your age and general health)
- Failure to improve your arm pain (less than 10% of cases)
- Leakage of spinal fluid from the spine (1%)
- Infection (1%)
- Damage to the nerve root or spinal cord (very rare, in the order of 1 in 1000-2000)
- Late instability of the spine ( rare, more common in multiple foraminotomies, or previous surgery to the spine)