Lumbar Laminectomy
Introduction
A lumbar laminectomy is an operation performed to decompress trapped nerves in the lumbar spine causing back pain and sciatica, or neurogenic claudication ( painful and numb legs on walking).
In order for the operation to have the maximum chances of success there has to be good evidence of nerve compression in the lumbar spine (preferably with an MRI scan), pain, weakness, or numbness in the leg or legs corresponding to the MRI findings
operation codes
For the purposes of your medical insurance you may need to quote the following codes to your insurer for pre-authorisation of treatment
V2560 Lumbar laminectomy – 1-2 Levels
V2562 Lumbar Laminectomy – 3 or more levels
V2542 Lumbar Foramenotomy
V2543 Revision Lumbar Foramenotomy
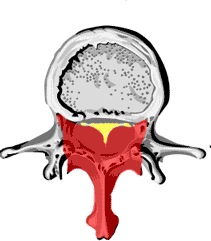
The pictures below show the diagram and MRI scan of a normal lumbar spine, and then a patient suffering with lumbar stenosis.

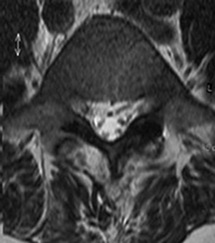

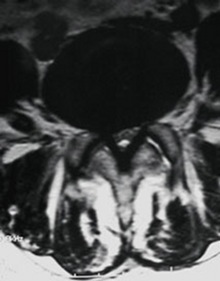
It is hopefully clear that the canal where the nerves run in the upper images ( white fluid with darker dots equating to nerves), is pinched tightly in the lower images, largely due to overgrowth of the facet joints and thickening of the yellow ligament.
The operation is performed to take pressure off the nerves trapped in the spinal canal (laminectomy) and as the nerves leave the spine to go to the legs (foraminotomy).
Making the operation minimally invasive
My own preference is to perform an operation called an ‘intersegmental decompression.’ This allows a smaller incision to be made on the back, and a more limited removal of the bone is performed, yet the nerves are still decompressed.
The operation is performed using a microscope, and the nerves are decompressed by removing the bone and ligament trapping them using a very small drill, and special instruments to remove small pieces of bone.
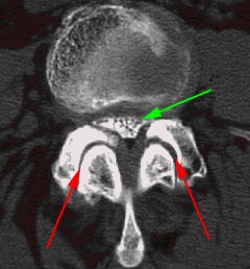
This image shows how the nerves (green arrow) are trapped by the enlarged facet joints (red arrows). The extra bone formed by wear and tear on the facet joints is removed, whilst sparing the joints themselves
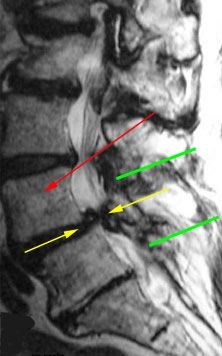
The above shows an MRI scan of lumbar canal stenosis between L4 and L5. The Red arrow indicates L4, the yellow arrows show the site of the stenosis, in this case due to a combination of disc prolapse from the front, and swelling of the yellow ligament and facet joints from the back. The green lines indicate the extent of the surgical approach, and likely extent of bone removal
Occasionally, in cases of large disc prolapse, a laminectomy, rather than a microdiscectomy approach is needed to be able to remove the disc safely.
The Operation
The operation is performed under a general anaesthetic
You will be lying on your front during the surgery. You will be lying in a special mattress which protects your skin, and your head supported in a jelly ring.
An X-Ray will be taken to localise very closely the site of surgery, this allows a small skin incision to be made just over the spinal level to be decompressed. For a single level lumbar laminectomy the incision is usually 6-8cm long (about 3 inchs)
In order to get to the spine the muscle attached to the spine has to be separated from the bone of the spine. The image above shows the extent of bone removal during a laminectomy operation. The red shaded area is the area of bone and yellow ligament that will be removed during surgery.
Once the bone of the spinous process and lamina is exposed, this bone is removed using bone cutting instruments together with the ‘yellow’ ligament that passes from the laminae above and below. The dura is the fibrous covering of the nerves in the spinal canal, and all attempts are made to remove the bone and ligament whilst avoiding tearing this layer. Once the spinal canal has been decompressed the microscope may be used to aid removal of bone around the nerve roots as they leave the spine to go to the legs.
At the end of the operation a drain may be left at the site of the operation. This is a thin silicone tube which allows drainage of any blood that collects in the wound into a plastic bottle, the drain is usually removed 24hrs after the operation. The wound is closed with stitches that absorb over time, and the skin often close with buried dissolving stitches and paper stitches.
This ‘lumbar laminectomy”:https://www.spine-health.com/video/lumbar-laminectomy-surgery-video?jwsource=cl by spine-health in The USA has a useful illustrative video explaining laminectomy that may be worth looking at.
Recovery From Surgery
Generally patients recover quickly from this operation. Because the operation involves stripping an area of muscle from the spine, the commonest problem is low back pain and stiffness after surgery. This may limit your walking immediately after surgery, however we encourage patients to get up as soon as you are comfortable, preferably the same afternoon or the morning after surgery. This pain tends to be well controlled with painkilling medication such as ibuprofen, or a morphine-based medication. The morning after your operation (or even sooner if you feel up to it) you will be encouraged to walk and use the bathroom with staff supervision, a physiotherapist will see you and supervise your mobilisation. Most patients will stay in hospital for 24-48 hours.
You can return to work when you fell comfortable, clearly this will depend upon how physically demanding your job is. In most cases 14 days off work is sufficient, if your job is physical then you may need up to 6 weeks off work. The DVLA state that you can drive when sufficiently recovered from surgery, in practical terms this means being able to look side to side and operate the car controls safely. Elderly patients may need additional support at home in the initial weeks after surgery. Thus, we would recommend getting additional family support if you are on your own at home, if this isn’t possible your GP may be able to organize some additional support for you
Results Of Surgery
The results of surgery are good with a 90+% rate of improving sciatica and symptoms of neurogenic claudication due to spinal stenosis
The operation is not aimed at improving back pain, this is because the back pain usually originated from the degenerative changes in the spine and the changes due to wear and tear cannot be reversed with surgery. Some back pain due to muscle spasm may well improve however
The risks of surgery include, but are not limited to:
The risks of a general anaesthetic ( this depends on your age and general health)
Failure to improve your leg pain (less than 10% of cases)
Leakage of spinal fluid from the spine (1%)
Infection (1%)
Damage to the nerve root or spinal nerves (very rare, in the order of 1 in 1000-2000), this can in theory result in weakness of the legs below the knees, and possibly incontinence
Late instability of the spine ( rare, more common in multiple level laminectomies, or previous surgery to the spine)